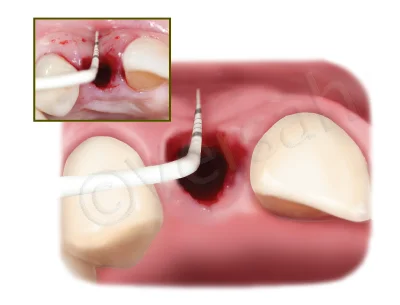
• EXTRACT DAMAGED TOOTH AND REMOVE GRANULATION TISSUE AND REMAINS OF PERIODONTAL TISSUE.
• USE THE DENSAH BURS IN OD MODE (CCW ROTATION) TO PREPARE THE IMPLANT SITE AND DENSIFY THE BONE BED.
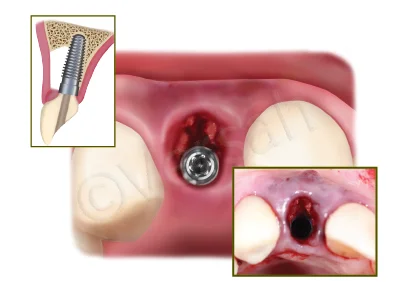
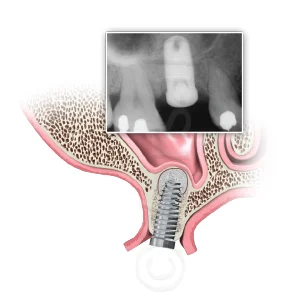
• ANCHOR THE IMPLANT INTO THE PALATAL WALL.
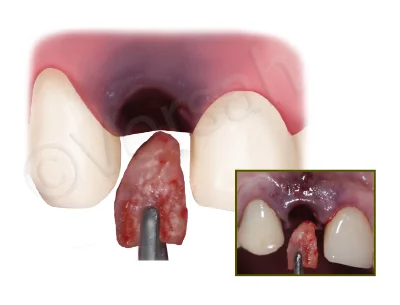
• HARVEST AND RESHAPE CORTICO-CANCELLOUS GRAFT AND PARTICULATE BONE FROM THE MAXILLARY TUBEROSITY. INSERT AND STABILIZE THE
CORTICO-CANCELLOUS AND PARTICULATE GRAFT INTO THE BUCCAL ASPECT OF THE RECEPTOR SITE.
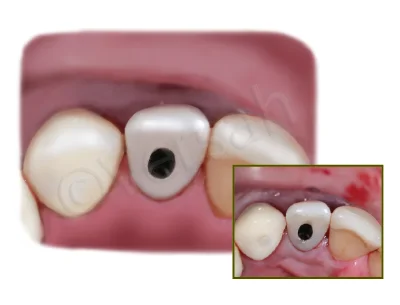
• PLACE A MANUFACTURED SCREW RETAINED PROVISIONAL RESTORATION WITH AN ADEQUATE EMERGENCE PROFILE. (CEMENTED RESTORATION
MUST NOT BE UTILIZED)
• ALLOW A MINIMUM 4 MONTHS HEALING AND PLACE A SCREW RETAINED FINAL PORCELAIN CROWN.